Entrustment and Entrustability Scales in CBD – Tips for Success!

Entrustment performance ratings (anchors) provide a meaningful structure around the day-to-day decisions physician supervisors already make about trainee performance. These decisions are rooted in the rater’s “trust” in a resident’s safe and independent practice ability.
Why use Entrustment Anchors instead of other Scales?
Entrustment anchors have been demonstrated to be more reliable than traditional anchors (below/meets/above expectations). Experience with entrustment anchors has also demonstrated that trainees are willing to accept lower scores if they also receive the concrete feedback required to improve performance.
Below are two examples of commonly used entrustment scales in Obstetrics and Gynaecology:
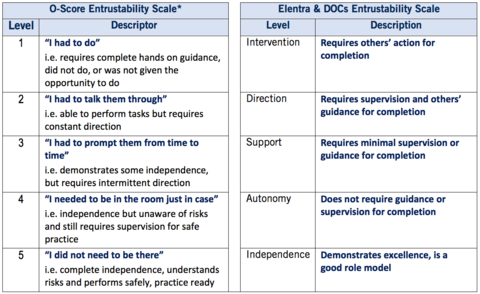
*Gofton WT, Dudek NL, Wood TJ, Balaa F, Hamstra SJ. The Ottawa surgical competency operating room evaluation (O-SCORE): a tool to assess surgical competence. Acad Med. 2012;87(10);1401-7.
Entrustment anchors such as “I had to talk them through” and “I did not need to be there” are used to rate a trainee’s ability to safely and independently perform practice activities without supervision. As indicated, at the high end of this performance scale, the observer’s “trust” in a trainee’s ability to independently and safely practice is closely linked with the trainee’s understanding of any real or potential risks involved in the activity.
To demonstrate “understanding” versus “awareness” of a risk involves not only verbalizing it but also taking the anticipatory actions required to mitigate or manage the event should it occur. For example, a resident might demonstrate that they understand the added risk in a patient with challenging anatomy by preparing backup equipment on the sterile procedure tray or first consulting another speciality, which seasoned experts do all the time.
When should I feel comfortable giving a level “5” or “Independence”?
It is important to appreciate that if you rate a trainee at a level “5” (or autonomy/independent), it does not mean the resident has achieved the EPA and is authorized to do this clinical task independently going forward (e.g. laparoscopic entry).
This rating reflects how the observer feels the resident managed this instance of the EPA or piece of the EPA and provides a piece of the information used by the competency committee to make a final determination about the resident’s EPA success.
Tips for Success!
- Remember that entrustment ratings involve judging a resident’s safe and independent practice ability on the basis of what you observed today. These ratings are NOT about predicting future performance.
- Measure observed performance against the standard of safe and independent practice, not to the stage of training the learner is at.
- Rating residents as independent does not mean that they are now allowed to always independently perform that task. It means that they were independent on this occasion.
Where can I find more information about Entrustment?
For more information on entrustment and how to use the Entrustability Scale, see the Entrustment module developed by the Royal College.
This tips sheet was adapted and excerpted from “Workplace-Based Assessment Implementation Guide: Formative tips for medical teaching practice” Royal College of Physicians and Surgeons of Canada:
Gofton, W, Dudek, N, Barton, G, and Bhanji, F. (2017). Workplace-Based Assessment Implementation Guide: Formative tips for medical teaching practice. 1st ed. (PDF) Ottawa: The Royal College of Physicians and Surgeons of Canada, pg. 1-12. Available at: Royal College of Physicians and Surgeons)
_____________________________________________________________
Don't want to miss a post? Follow us on social media for more news!
FACEBOOK | INSTAGRAM | TWITTER
If you would like to be a guest blogger, please contact us at obgyn@utoronto.ca.